Let’s fix your Heartburn.
The New Heartburn Center at VHC Health Opened in the Summer of 2023
When fluid from your stomach moves backwards into your esophagus, throat and lungs, pain and other problems occur. Unfortunately, patients and clinicians use many different names do describe the same basic process so confusion about what you have and how to treat it understandable. Acid reflux, Gastroesophageal Reflux Disease (GERD), Heartburn, LPR, Dyspepsia, Hiatal Hernia, Indigestion, Non-cardiac chest pains, esophageal spasms are all terms that are used to label the symptoms that result from the backwards movement of the highly irritating stomach contents into the chest and esophagus.
Since reduction of the naturally occurring acid in the stomach fluid makes some of the symptoms less intense patients mistakenly begin to think that acid is the “enemy”. It is not. Patients who have GERD issues typically do not make more gastric acid than their friends who have no symptoms. Often, they have problems with their anatomy that allows the “valve/sphincter” between their stomach and esophagus to leak. It’s a plumbing problem not an acid problem. The most common anatomic problem is a hiatal hernia which allows the upper stomach to slide through the diaphragm and into the chest which disrupts the integrity of your natural valve.
We need acid in our stomach to help us digest our food and to protect us from infections. The reduction of acid in the stomach is a double edge sword. It may help us feel better and reverse some of the damage that the acid has caused in our esophagus but there can be consequences when taken for extended periods of time. People may feel better with less burning on the medications, but the reflux continues to occur, and you may continue to have symptoms like regurgitation.
When PPIs such as Nexium, Prilosec and Prevacid first came to market, they were celebrated by many suffering from Acid Reflux or GERD. They offered relief of heartburn to many people with seemingly few side effects. The medications were believed so safe that the FDA allowed them to go over the counter in 2003, available to the public without a prescription.
The directions for PPI use are for 14 days up to 3 times a year. Although many people have taken these medications for years they are not indicated for everyday use. Since GERD is caused by a defective valve, unless you fix that valve, 14 days of a medication will only help for those 14 days. When you stop the medications, your valve is still not working, and so your symptoms will return.
Now that there have been patients taking these medications for years, we have a little more insight into the long-term problems with the medications.
Some of the long-term problems associated with PPIs identified by medical research include: click on the links below
- Changing gut ecology
- Heart attacks
- Dementia
- Osteoporosis
- Kidney disease
- Pneumonia
- Vitamin and mineral deficiency
In short, Acid belongs in the stomach. The only way to keep the acid in the stomach and not suffer from GERD is to fix the valve between the stomach and esophagus. There are several procedures available today that can accomplish this. The most durable results require significant surgical expertise and experience and are achieved with the following procedures. They are generally done as an outpatient procedure or with a short over-night stay.
Fundoplication – This is the classic “gold standard” procedure that has been utilized for 5 decades to control reflux. It is now done with laparoscopic and Robotic approaches depending on surgeon preference. If a hiatal hernia is present, it is repaired, and the upper portion of the stomach is wrapped around the lower esophagus to apply pressure and to prevent reflux. This essentially creates a new one-way valve to control reflux, but this does make it harder to belch and vomit after surgery.
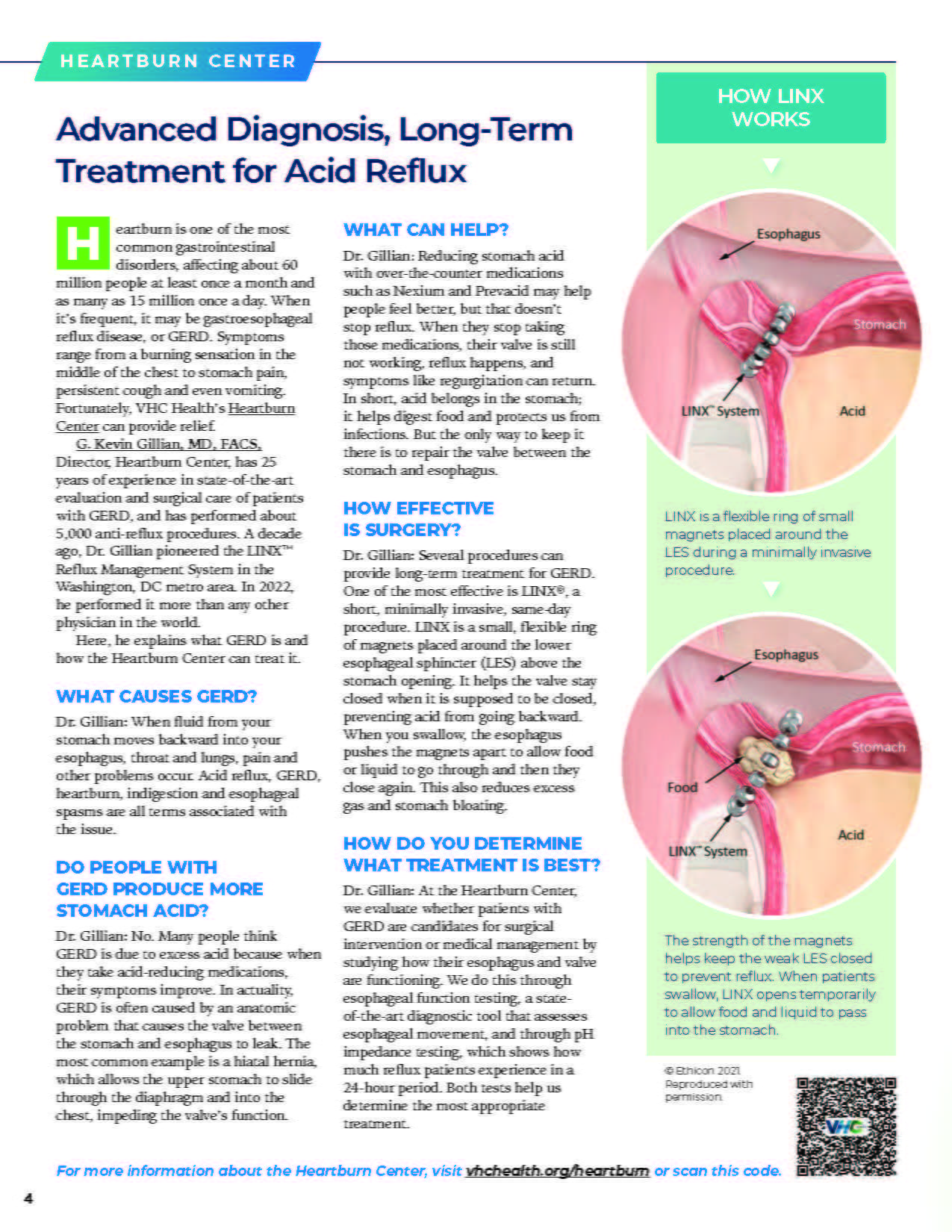
LINX procedure – This is a newer laparoscopic/Robotic procedure where a hiatal hernia is fixed if present, and a small ring of magnets is placed around the valve between the stomach and esophagus. This helps your valve stay closed when it is supposed to be closed. When you swallow, the esophagus pushes the magnets apart and allows the food/liquid to go through and then closes again. Unlike the Fundoplication this acts more like your normal valve, so it is easier to belch and vomit. Consequently, bloating is excess flatus is reduced too. This lowered side effect profile has made this an increasingly popular option for patients.
Heartburn Center
Part of the process of evaluating patients with GERD for surgical intervention or to maximize their medical management involves getting accurate data about how well their esophagus/valve is functioning and whether someone’s symptoms are truly related to reflux events. Acquiring this data and knowing what to do with it allows clinicians to maximize control and minimize symptoms in their patients. It also allows the surgeon to match the patient to the most appropriate surgery.
Dr. Gillian established his first dedicated Heartburn Center in the area nearly 25 years ago to ensure that patients from referring clinicians could get the most accurate diagnosis of their GERD and swallowing disorders. The newly renovated Heartburn Center at VHC continues that mission. The studies performed here are ordered by your clinicians to help diagnose the cause of swallowing problems, sore throats, chest pain, chronic cough, and determine why some people are not responding to standard GERD therapy.
Heartburn Center Studies
Esophageal Function Testing (EFT) also goes by other names such as High-Resolution Impedance Manometry (HRIM) – This is a state-of-the-art diagnostic tool to evaluate esophageal motility patterns to facilitate the diagnosis and management of swallowing disorders. It is also used to guide surgeons on the intensity of their repairs.
24-hour pH Impedance Testing focuses on whether GERD is playing a role in the patients’ symptoms. It allows us to determine how much reflux is occurring in the esophagus as the patient moves through their daily activities, meals, and sleep. We can determine the volume of reflux, how much of it is acidic and whether it is correlating with the patient’s symptoms. Sometimes we learn that people are failing medical management of GERD because the diagnosis was wrong, and they never had acid reflux.
G. Kevin Gillian, MD, FACS is the Director of the Heartburn Center. He has been providing state of the art surgical care and evaluation of patients with GERD and esophageal motility problems for 25 years. He has performed nearly 5000 anti-reflux procedures and has been offering the LINX procedure now for nearly a decade. He was #1 in the world in 2022 for number of LINX cases performed and he continues to train surgeons around the country in the evaluation and surgical care of patients with GERD issues.
If you are interested in eliminating or improving the control of you GERD and swallowing issues Dr. Gillian and his team at the VHC Heartburn Center are ready to help. Just reach out to us or have your clinician contact us.